 Share on Facebook
Share on Facebook
 You know the official story: Covid-19 is a highly contagious and deadly infection that can be stopped only by social distancing, frequent handwashing, lockdowns, masks, mass testing, contact tracing and ultimately vaccines. But in reality, Covid-19 appears to be a highly contagious, dangerous, lab-manufactured “trigger” for the preexisting conditions of an aging and increasingly chronically ill population.
You know the official story: Covid-19 is a highly contagious and deadly infection that can be stopped only by social distancing, frequent handwashing, lockdowns, masks, mass testing, contact tracing and ultimately vaccines. But in reality, Covid-19 appears to be a highly contagious, dangerous, lab-manufactured “trigger” for the preexisting conditions of an aging and increasingly chronically ill population.
The virus itself isn’t the primary cause of most Covid-19 hospitalizations and fatalities. Rather, the virus exploits other serious diseases with high mortality that are widespread in the population and dangerous in and of themselves. It’s these comorbidities, along with rampant medical malpractice, that are the main drivers of Covid-19 hospitalizations and deaths. To put it simply: People are dying with Covid-19 as opposed to dying from it.
To understand the truth versus the official story, we have to separate the real statistics from the “official” statistics on cases, hospitalizations and deaths from Covid-19. A relatively high “case” load does not mean people are actually getting sick and dying. The media has been conflating a positive test result with the actual disease, thereby deliberately misleading the public into believing the infection is far more serious and widespread than it actually is.
Covid-19 is not confirmed by a positive test; it is a clinical diagnosis of someone infected with SARS-CoV-2 who is exhibiting severe respiratory illness characterized by fever, coughing and shortness of breath. By using a test that falsely labels healthy individuals as sick and infectious, mass testing drives the narrative that we’re in a lethal pandemic.
Indeed, the use of reverse-transcription polymerase chain reaction (RT-PCR) tests is at the very heart of this entire scam. If it wasn’t for this flawed test, there would be no pandemic to speak of.
Mislabeled causes of death
According to groundbreaking data released by the US Centers for Disease Control and Prevention (CDC) on August 26, 2020, only 6 percent of the total Covid-19-related deaths in the US had Covid-19 listed as the sole cause of death on the death certificate.1
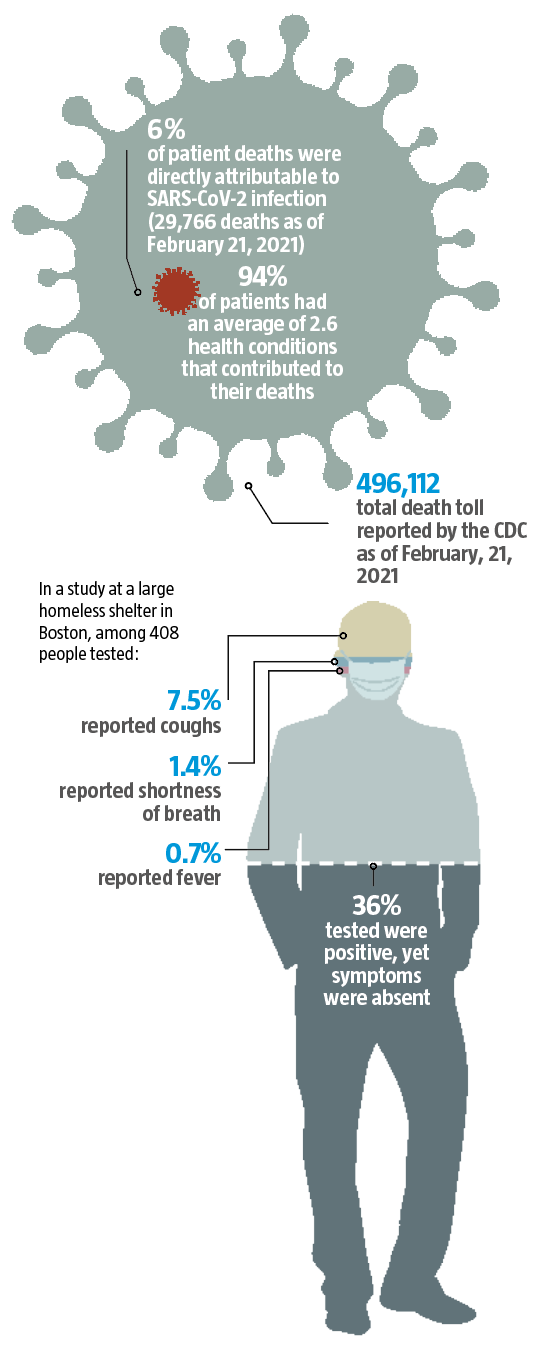
To help that sink in: 6 percent of 496,112 (the total death toll reported by the CDC as of February, 21, 2021) is 29,766. In other words, SARS-CoV-2 infection was directly responsible for 29,766 deaths of otherwise healthy individuals—a far different story from the 200,000-plus (and rising) number reported in the media. The remaining 94 percent of patients had an average of 2.6 health conditions that contributed to their deaths.
There are several major aspects of the official “scientific” narrative on the nature, infectivity and virulence of Covid-19 that are deliberately misleading and spreading panic among the public. These include the use of faulty, miscalibrated PCR lab tests that artificially inflate the number of Covid-19 cases.
The fact is, a vast majority of those who test positive for SARS-CoV-2 remain asymptomatic and are highly unlikely to spread the disease to others. They simply aren’t sick. The PCR test is merely picking up inactive (noninfectious) viral particles.
In one study, which looked at pregnant women admitted for delivery, 87.9 percent of the women who tested positive for the presence of SARS-CoV-2 had no symptoms.2
Another study looked at a large homeless shelter in Boston. Of 408 people tested, 147 (36 percent) were positive, yet symptoms were conspicuously rare. Cough occurred in only 7.5 percent of cases, shortness of breath in 1.4 percent, and fever in 0.7 percent. All symptoms were “uncommon among Covid-positive individuals,” the researchers noted.3
A study in Nature Communications assessed the risk posed by asymptomatic people by looking at the data from a mass screening program in Wuhan, China. The city had been under strict lockdown between January 23 and April 8, 2020. Between May 14 and June 1, 2020, 9,899,828 residents of Wuhan city over the age of six underwent PCR testing. Of these, 9,865,404 had no previous diagnosis of Covid-19, and 34,424 were recovered Covid-19 patients.
In all, there were zero symptomatic cases and only 300 asymptomatic cases detected. (The overall detection rate was 0.3 per 10,000.) Importantly, not a single one of the 1,174 people who had been in close contact with an asymptomatic individual tested positive.
Additionally, of the 34,424 participants with a history of Covid-19, 107 individuals (0.310 percent) tested positive again, but none were symptomatic. As noted by the authors, “Virus cultures were negative for all asymptomatic positive and repositive cases, indicating no ‘viable virus’ in positive cases detected in this study.” Interestingly, when they further tested asymptomatic patients for antibodies, they discovered that 190 of the 300 (63.3 percent) had actually had a “hot” or productive infection resulting in the production of antibodies, yet none of their contacts had been infected. In other words, even though asymptomatic cases were (or had been) carriers of apparently live virus, they still did not transmit it to others.4
Another misleading practice is to conflate statistics on deaths. Some 94 percent of so-called Covid-19 deaths were people who died with Covid-19, as they had other preexisting chronic diseases or comorbidities.1 The idea that Covid-19 is a lethal pandemic is also disproven by all-cause mortality statistics, which show mortality has remained steady during 2020 and doesn’t veer from the norm.5
Other fearmongering tactics include public statements exaggerating the threat of Covid-19 to children, youth and students, as well as the risk of youth to spread Covid-19 to teachers and older adults in general. Even the Chief Medical Advisor to the President, Dr Anthony Fauci, now admits that students pose little or no threat to teachers or older adults and that schools should be reopened.6
How the PCR test works
The PCR swab collects RNA from your nasal cavity. This RNA is then reverse-transcribed into DNA. Due to its tiny size, it must be amplified to become discernible. Each round of amplification is called a cycle, and the number of amplification cycles used by any given test or lab is called a cycle threshold (CT).
The higher the CT, the greater the risk that insignificant pieces of viral DNA end up being magnified to the point that the test reads positive even if your viral load is extremely low or the virus is inactive and poses no threat to you or anyone else.
Many scientists have noted that anything over 35 cycles is scientifically indefensible.1 Even Dr Anthony Fauci, a leading proponent of gain-of-function experiments and mandatory vaccines, has admitted that the chances of a positive PCR result being accurate at 35 cycles or more “are minuscule.”
Faulty PCR-positive test results
News reports or public health proclamations on Covid-19 are often accompanied by ominous graphs, always trending upward, with dire warnings of a “second or third wave” of mass hospitalizations and deaths being imminent if people don’t hunker down, obey authority and isolate themselves as thoroughly as they did in the early stages of the pandemic.
In the fine print of these alarming news reports, there are often admissions that while actual deaths from Covid-19 have declined, we can expect massive deaths if people stop wearing masks or resume a semblance of normal life. The upbeat news of these scare articles is that the danger of infection and death will eventually subside once everyone gets vaccinated.
But we need to ask ourselves: What do these experts and media outlets actually mean by an increasing number of “cases” of Covid-19?
As former New York Times reporter Alex Berenson points out in his book Unreported Truths About Covid-19 and Lockdowns: “A ‘case’ of coronavirus points only to a positive test result . . . It does not mean that a person will become sick—much less that he or she will be hospitalized, need intensive care, or die.”7
At present, the PCR test is the primary method used to test people for Covid-19. The problem with that is twofold. First of all, the PCR test cannot distinguish between inactive viruses and “live” or reproductive ones.8 This is a crucial point, since inactive and reproductive viruses are not interchangeable in terms of infectivity. If you have a nonreproductive virus in your body, you will not get sick and you cannot spread it to others. For this reason, the PCR test is grossly unreliable as a diagnostic tool. Second, many if not most laboratories amplify the RNA collected far too many times, which results in healthy people testing positive. In order for the PCR test to be of any use whatsoever in terms of diagnosing Covid-19, labs would need to considerably reduce the number of amplification cycles used (see box, left).
A September 28, 2020, study in Clinical Infectious Diseases revealed that when you run a PCR test at a CT of 35 amplification cycles or higher, the accuracy drops to 3 percent, resulting in a 97 percent false positive rate.9 Yet tests recommended by the World Health Organization are set to 45 cycles,10 and the US Food and Drug Administration and the CDC recommend running PCR tests at a CT of 40 cycles.8
The question is why, considering the consensus is that a CT over 35 renders the test useless. When labs use these excessive cycle thresholds, you clearly end up with a grossly overestimated number of positive tests, so what we’re really dealing with is a “casedemic”—an epidemic of false positives.11
As noted by author and investigative journalist Jon Rappoport: “All labs in the US that follow the FDA guideline are knowingly or unknowingly participating in fraud. Fraud on a monstrous level. . . Millions of Americans are being told they are infected with the virus on the basis of a false positive result, and . . .The total number of Covid cases in America—which is based on the test—is a gross falsity. The lockdowns and other restraining measures are based on these fraudulent case numbers . . .”12
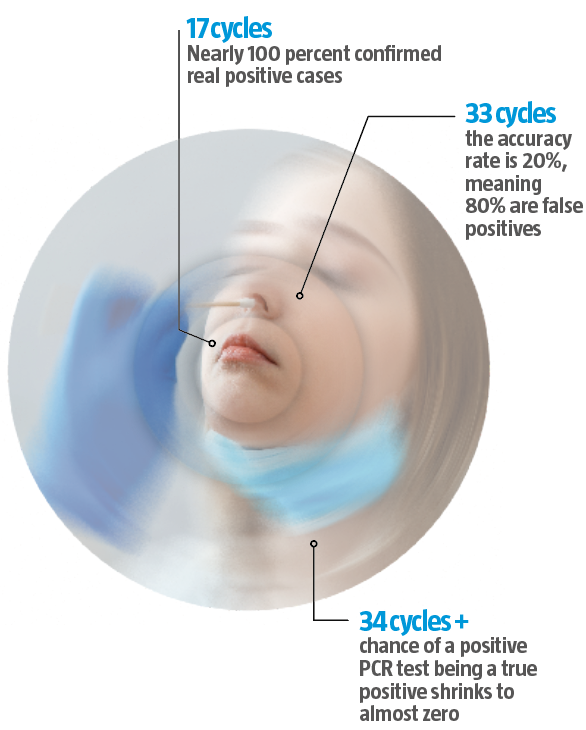
An April 2020 study in the European Journal of Clinical Microbiology and Infectious Diseases showed that to get 100 percent confirmed real positives, the PCR test must be run at 17 cycles. Above 17 cycles, accuracy drops dramatically.13
By the time you get to 33 cycles, the accuracy rate is a mere 20 percent, meaning 80 percent are false positives. Beyond 34 cycles, your chance of a positive PCR test being a true positive shrinks to almost zero. According to a December 3, 2020, systematic review published in the journal Clinical Infectious Diseases, no live viruses could be found in cases where a positive PCR test had used a CT above 24.14
What these studies show, then, is that if you actually have symptoms of Covid-19 and test positive using a PCR test that was run at 35 amplification cycles or higher, then you’re probably infected and likely infectious. However, if you do not have symptoms, yet test positive using a PCR test run at a CT of 35 or higher, then it is likely a false positive, and you pose no risk to others as you’re unlikely to carry any live virus.
In fact, provided you’re asymptomatic, you’re unlikely to be infectious even if you test positive with a test run at 24 CTs or higher.
According to Stephen A. Bustin, professor of molecular medicine and a world-renowned expert on the PCR test, when you get a positive result using a CT of 35 or higher, you’re looking at the equivalent of a single copy of viral DNA, and the likelihood of that causing a health problem is minuscule.15
In December 2020, Florida became the first US state to require labs to report the cycle threshold used for their PCR tests.16 In Europe, meanwhile, a court in Portugal has ruled that the PCR test is “not a reliable test for SARS-CoV-2, and therefore any enforced quarantine based on the results is unlawful.”17 China addressed the PCR problem by simply stopping testing people for Covid-19 except for those actually exhibiting symptoms.
An argument has been made for confirmatory molecular sequencing in a petition to the European Medicines Agency to put a halt to Covid-19 vaccine trials that are using misleading PCR tests.18
In the fall of 2020, according to epidemic and anthrax expert Dr Meryl Nass: “Without fanfare, the CDC acknowledged on another webpage that even if Covid was not listed by the doctor as the underlying cause of death, or the proximate cause of death, as long as it was listed as one cause or contributor, it would be coded as the cause of death.”
Indeed, the CDC website at the time of this writing reads (emphasis ours): “When Covid-19 is reported as a cause of death on the death certificate, it is coded and counted as a death due to Covid-19.”19
All these machinations with the death certificates hide the fact that the death rate from Covid-19 for everyone except those over 60 is significantly lower than the death rate for influenza.
Covid versus influenza
Research looking at the fatality ratio for the average person, excluding those residing in nursing homes and other long-term care facilities, presented September 2, 2020, in the Annals of Internal Medicine: “The overall noninstitutionalized infection fatality ratio [for Covid-19] was 0.26 percent . . . Persons younger than 40 years had an infection fatality ratio of 0.01 percent; those aged 60 or older had an infection fatality ratio of 1.71 percent.”20
Other sources are reporting similar findings. During an August 16, 2020, lecture at the Doctors for Disaster Preparedness convention, Dr Lee Merritt pointed out that, based on deaths per capita—the only way to get a true sense of the lethality of this disease—the death rate for Covid-19 at that time was around 0.009 percent.21 That number was based on a global total death toll of 709,000, and a global population of 7.8 billion. This also means the average person’s chance of surviving an encounter with SARS-CoV-2 was 99.991 percent.
In comparison, the estimated infection fatality rate for seasonal influenza listed in the Annals of Internal Medicine paper is 0.8 percent. Other sources put it a little higher. In either case, the only people for whom SARS-CoV-2 infection is more dangerous than influenza are those over the age of 60. All others have a lower risk of dying from Covid-19 than they have of dying from the flu.
Former White House coronavirus task force coordinator Dr Deborah Birx also confirmed this far lower than typically reported mortality rate when she, in mid-August 2020, stated that it “becomes more and more difficult” to get people to comply with mask rules “when people start to realize that 99 percent of us are going to be fine.”22
Class-action lawsuits
In early October 2020, an international team of class-action lawyers, led by Reiner Fuellmich, announced they will soon be filing lawsuits against a number of governments for utilizing imprecise PCR and antibody tests—which generate huge profits for Big Pharma as well as vaccine and testing companies—and then knowingly using the data from these faulty tests to justify lockdowns and suspensions of basic civil liberties, resulting in massive damage to public health, businesses, and citizens.1
As Fuellmich states, PCR tests, according to the leaflets that accompany the test kits, should not be considered true diagnostic tests for the presence of disease. Even the CDC admitted in a July 13, 2020, statement that PCR tests “may not necessarily indicate the presence of an infectious virus,” “may not prove that a SARS-CoV-2 fragment is the cause of clinical symptoms,” and cannot rule out diseases caused by other bacterial or viral pathogens.2
A September 20, 2020 “Open Letter from Medical Doctors and Health Professionals to All Belgian Authorities and All Belgian Media” reiterates some of the serious shortcomings of the PCR tests that are currently relied on to make the alarming claim that cases are rising across the US, Europe and the world: “The test does not measure how many viruses are present in the sample. A real viral infection means a massive presence of viruses, the so-called virus load. If someone tests positive, this does not mean that that person is clinically infected, is ill or is going to become ill.”3
Since a positive PCR test cannot reliably or automatically indicate active infection or infectivity, there’s absolutely no justification for the social measures taken, as they are based solely on these tests.
Comorbidities are the primary cause
To be fair, the official story and statistics have reported that underlying health conditions such as obesity, heart disease and diabetes are key factors in Covid-19 fatalities. Yet the data show they’re more than contributing factors: they’re the primary drivers of hospitalizations and deaths.
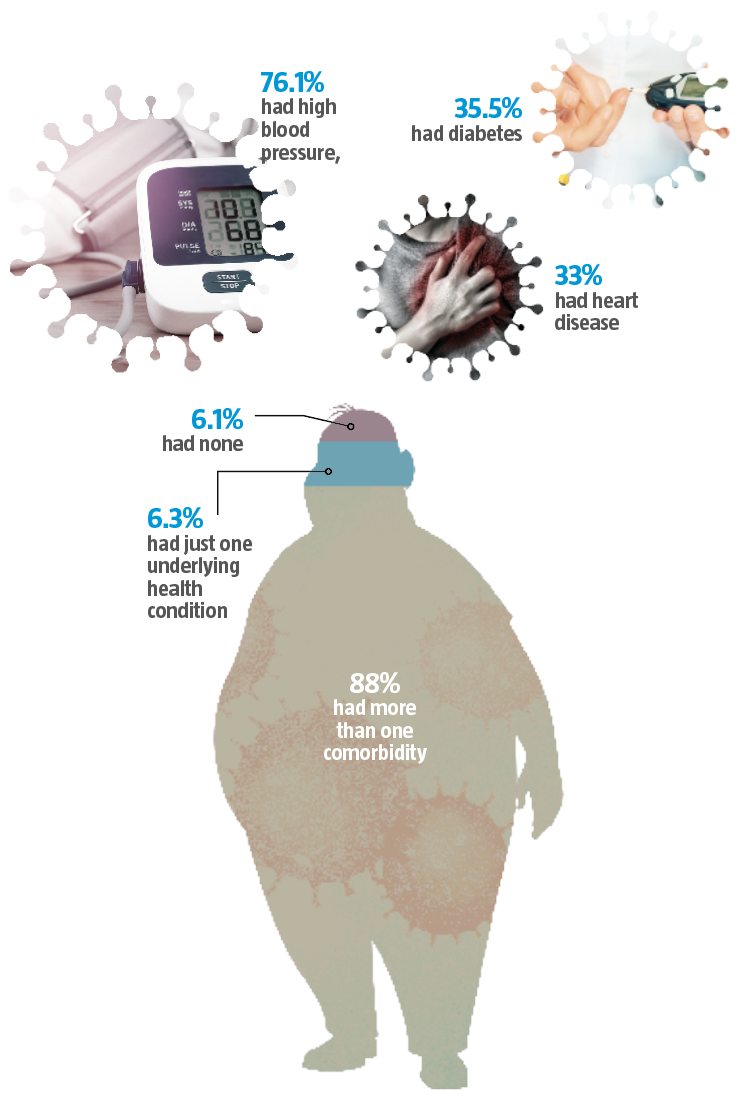
In one study, more than 99 percent of people who died from Covid-19-related complications had underlying medical conditions. Among those fatalities, 76.1 percent had high blood pressure, 35.5 percent had diabetes and 33 percent had heart disease.1
Another study revealed that among 18- to 49-year-olds hospitalized due to Covid-19, obesity was the most prevalent underlying condition, just ahead of hypertension.2 What’s more, investigations reveal that most Covid-19 patients have more than one underlying health issue. A study looking at 5,700 New York City patients found that 88 percent had more than one comorbidity. Only 6.3 percent had just one underlying health condition, and 6.1 percent had none.3
Most chronic conditions—particularly diabetes and high blood pressure—have roots in metabolic dysfunction, as people with metabolic dysfunction have compromised immune systems.
The common thread connecting nearly all of the Covid-19 comorbidities is insulin resistance. Insulin resistance is largely related to the transition to industrially processed foods and a reliance on carbohydrates over healthy fats.
This excerpt is adapted from Dr Joseph Mercola and Ronnie Cummins’ new book The Truth About Covid-19: Exposing the Great Reset, Lockdowns, Vaccine Passports, and the New Normal (Chelsea Green Publishing, April 2021). Reprinted with permission from the publisher.
https://www.wddty.com/features/the-truth-behind-the-covid-statistics/?utm_medium=email&utm_source=wddty&utm_content=The+truth+behind+the+Covid+statistics&utm_campaign=FREE+MEMBERS+enews+-+%28The+truth+behind+the+Covid+statistics%29+17.06.2021
|
References |
|
|
1 |
US Centers for Disease Control and Prevention, “Provisional Death Counts for Coronavirus Disease 2019,”updated December 9, 2020, www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm. |
|
2 |
N Engl J Med, 2020; 382: 2163–64 |
|
3 |
medRxiv 2020.04.12.20059618; doi: https://doi.org/10.1101/ 2020.04.12.20059618 |
|
4 |
Nat Commun, 2020; 11: 5917 |
|
5 |
Lee Merritt MD, “SARS-CoV-2 and the Rise of Medical Technocracy,” August 16, 2020 (video), DDP 38th Annual Meeting, Las Vegas, Nevada, approximately 8 minutes in (Lie No. 1: Death Risk), www.bitchute.com/video/bhwyZqSv1h6g/; DG Rancourt, “All-Cause Mortality During Covid-19: No Plague and a Likely Signature of Mass Homicide by Government Response,” June 2020, www.doi.org/10.13140/RG.2.24350.77125; The Johns Hopkins News-Letter, “A Closer Look at US Deaths Due to Covid-19,” November 22, 2020 (archived), web.archive.org/web/20201126163323/https:/www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19 |
|
6 |
Mercola.com, “Fauci Says Schools Should Try to Stay Open,” December 27, 2020, blogs.mercola.com |
|
7 |
Alex Berenson, Unreported Truths About Covid-19 and Lockdowns (New Jersey: Bowker, 2020), 20. |
|
8 |
US Centers for Disease Control and Prevention, “CDC 2019 Novel Coronavirus RT-PCR Diagnostic Panel,” July 13, 2020, www.fda.gov/media/134922/download |
|
9 |
Clin Infect Dis, 2020; ciaa1491 |
|
10 |
World Health Organization, “Diagnostic Detection of Wuhan Coronavirus 2019 by Real-Time RT-PCR, January 13, 2020,” January 13, 2020, www.who.int; Euro Surveill, 2020; 25: 2000045 |
|
11 |
Association of American Physicians and Surgeons, “Covid-19: Do We Have a Coronavirus Pandemic, or a PCR Test Pandemic?” October 7, 2020, aapsonline.org |
|
12 |
Jon Rappoport, “Smoking Gun: Fauci States Covid Test Has Fatal Flaw; Confession from the ‘Beloved’ Expert of Experts,” November 6, 2020, blog.nomorefakenews.com |
|
13 |
Eur J Clin Microbiol Infect Dis, 2020; 39: 1059–61 |
|
14 |
Clin Infect Dis, 2020; ciaa1764 |
|
15 |
The Infectious Myth, “Stephen Bustin on Challenges with RT-PCR,” April 14, 2020, https://www.youtube.com/watch?v=fkSps-RSNMo |
|
16 |
Florida Health, “Mandatory Reporting of Covid-19 Laboratory Test Results: Reporting of Cycle Threshold Values,” December 3, 2020, www.flhealthsource.gov/files/Laboratory-Reporting-CT-Values-12032020.pdf |
|
17 |
The Portugal News, “Covid PCR test reliability doubtful – Portugal judges,” November 27, 2020, www.theportugalnews.com |
|
18 |
Drs Wolfgang Wodarg and Michael Yeadon, “Petition/Motion for Administrative/Regulatory Action Regarding Confirmation of Efficacy End Points and Use of Data Connection with the Following Clinical Trial(s),” December 1, 2020 (PDF), www.wodarg.com/app/download/9033912514/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_signed_with_Exhibits_geschwa%CC%88rzt.pdf?t=1606870652 |
|
19 |
US National Center for Health Statistics, “Covid-19 Death Data and Resources,” accessed December 8, 2020, www.cdc.gov/nchs/nvss/covid-19.htm |
|
20 |
Ann Intern Med, 2021; 174: 135–6 |
|
21 |
Lee Merritt, MD, “SARS-CoV2 and the Rise of Medical Technocracy,” August 16, 2020 (video), DDP 38th Annual Meeting, Las Vegas, Nevada, www.bitchute.com/video/bhwyZqSv1h6g/ |
|
22 |
El Dorado News-Times, “Birx Says Country Weary of Covid-19, Recognizes Arkansas’ Improvement During Visit,” August 18, 2020, www.eldoradonews.com |
How the PCR test works
|
References |
|
|
1 |
Vaccine Reaction, “Coronavirus Cases Plummet When PCR Tests Are Adjusted,” September 29, 2020, thevaccinereaction.org |
|
2 |
Jon Rappoport, “Smoking Gun: Fauci States Covid Test Has Fatal Flaw; Confession from the ‘Beloved’ Expert of Experts,” November 6, 2020, blog.nomorefakenews.com; This Week in Virology 641 (July 16, 2020), “Covid-19 with Dr. Anthony Fauci,” youtu.be/a_Vy6fgaBPE?t=260. |
Comorbidities are the primary cause
|
References |
|
|
1 |
EpiCentro, “Report Sulle Caratteristiche dei Pazienti Deceduti Positivi a Covid-19 in Italia Il Presente Report è Basato sui Dati Aggiornati al 17 Marzo 2020,” March 17, 2020, www.epicentro.iss.it/coronavirus/bollettino/Report-Covid-2019_17_marzo-v2.pdf. |
|
2 |
MMWR Morb Mortal Wkly Rep 2020; 69: 458–64 |
|
3 |
JAMA, 2020; 323: 2052–9 |
Class-action lawsuits
|
References |
|
|
1 |
Reiner Fuellmich, “The Corona Fraud Scandal Must Be Criminally Prosecuted for Crimes Against Humanity.” October 9, 2020; news.fiar.me |
|
2 |
CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel,” revised and updated December 1, 2020, www.fda.gov/media/134922/download |
|
3 |
Docs 4 Open Debate, “Open Letter from Medical Doctors and Health Professionals to All Belgian Authorities and All Belgian Media,” September 5, 2020, docs4opendebate.be/en/open-letter |


